As I write this, I’ve just started my sixth cycle of chemo. Each cycle is 3 weeks and goes something like:
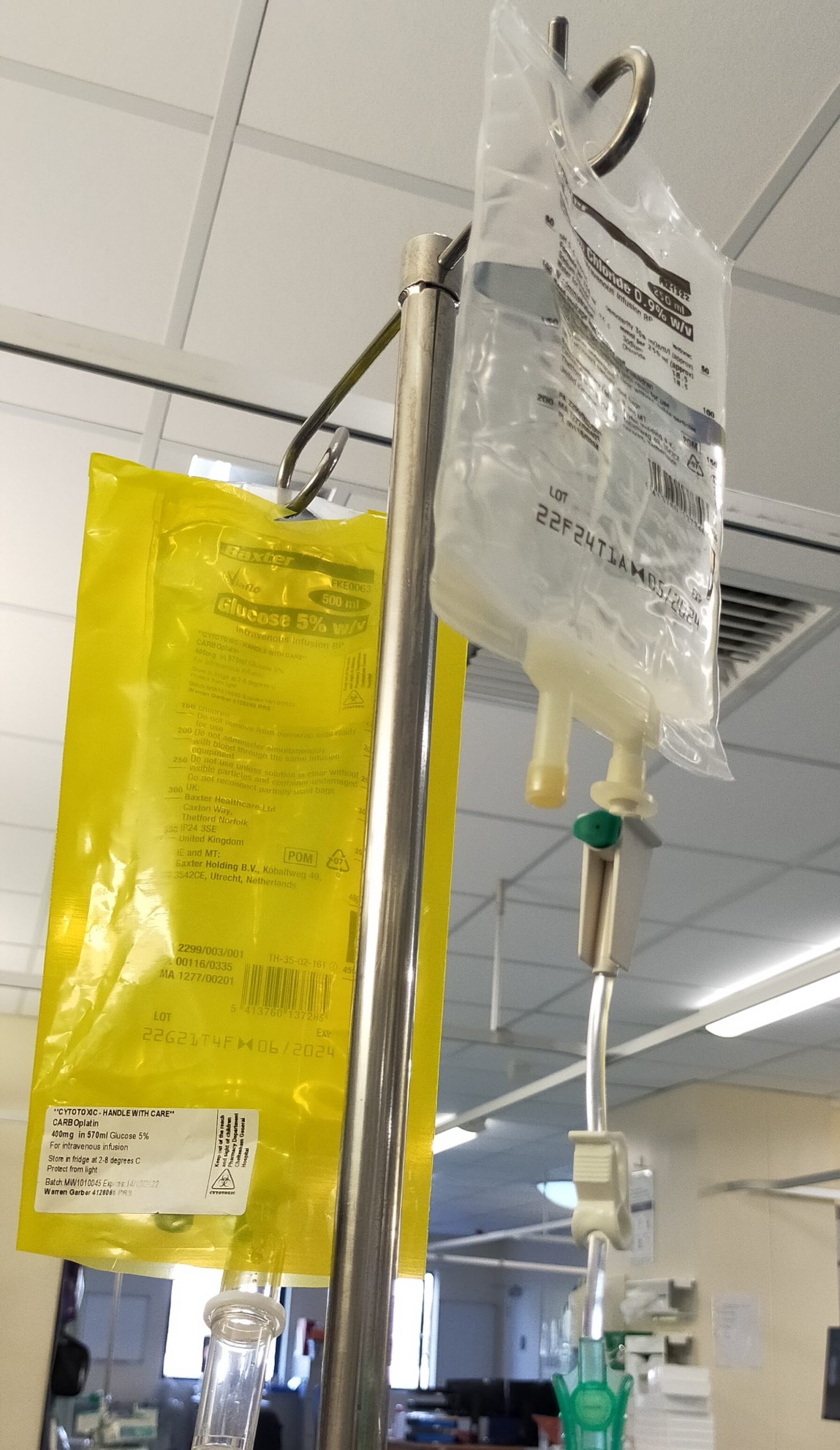
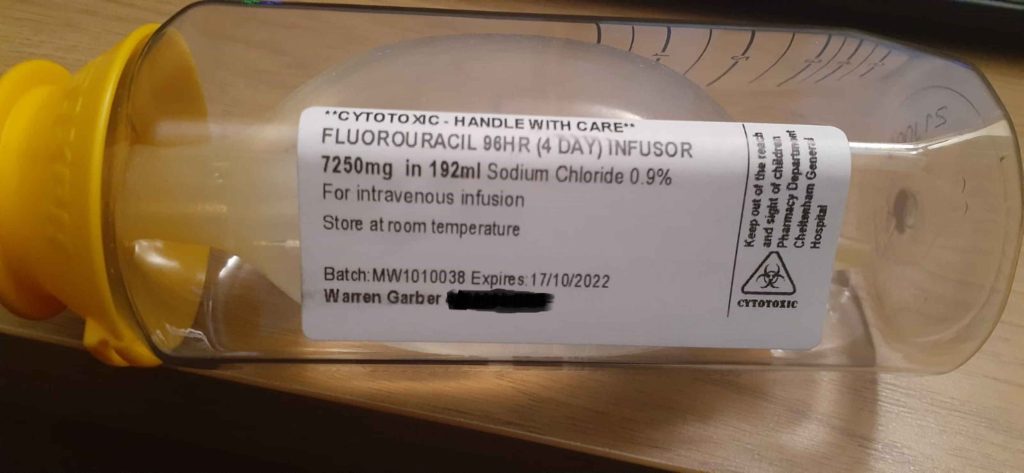
Week 1 (Mondays) - I get two infusions in hospital – Carboplatin and Fluoroucil 5FU along with anti-sickness medication and Dexamethasone steroid, which I also get tablets to take at home.
Week 2 – No new infusions or drugs, just feel the treatments working (feeling of fatigue and occasional sickness), along with forgetfulness which I blame on the chemo, but really I suppose it’s a function of age ☹
Week 3 – This is a so-called recovery week where my body regains its white blood cells and has increased immunity from infection.
At the end of Week 3, I’m back in hospital on the Friday for blood samples and the consultant checks that I’m fit and well enough to start the poisoning cycle again on the following Monday!
So, being in my sixth cycle of chemo, I think this is the last for now. The regimen calls for six cycles of 3 weeks (18 weeks total) and then evaluation of the treatment and its success (or not) of slowing the growth of existing tumours and any spread to further parts of the body.
Evaluation is done by taking CT scans, which I had at the end of September and then my consultant Dr Grant, decides on the next steps. This could be more of the same to follow-on, a break in chemo and then restart when my body recovers or a completely different treatment.
That was a simple enough paragraph to write, but the actuality is more complex and frustrating.
It seems that post-covid the NHS are under pressure to increase scanning for many patients, especially those with cancer (or initial scans to find out) – and this appears to be happening 7 days a week here. This is the good news.
The not so good news is that the next step in the chain is the ‘Radiologist Principal Interpreter’ (as they’re called here in Gloucestershire), to write a report detailing what the scans show. It is this report that goes to my consultant for him to decide on prognosis and treatment.
But now we’re in a position that the Radiologists are completely overwhelmed with the higher volume of scans to interpret, meaning there are lengthy delays in getting these to the consultant.
Which is where I’m at right now – with no report available after almost 3 weeks and not knowing how I’m doing, or what happens next.
Hoping to know more soon(ish) and write an update on this in a week or so.